Status epilepticus - continuous or rapid sequential seizure activity for 30 minutes or more - is a medical emergency with a high mortality rate in both children and adults. Prompt and effective treatment is key; therefore the American Epilepsy Society (AES) has released a new guideline to help physicians, hospitals, and health systems treat patients effectively. The guideline is published in the January/February issue of Epilepsy Currents, the AES journal.
Each year, between 50,000 and 150,000 Americans have status epilepticus with rates of death estimated at less than 3 percent for children and up to 30 percent for adults. This guideline focuses on convulsive status epilepticus in particular because it is the most common type of status epilepticus and is associated with substantial mortality.
"This is a valuable new guideline for both children and adults that could change the approach many clinicians take in treating these seizure emergencies," said guideline author Tracy Glauser, M.D., with Cincinnati Children's Hospital Medical Center's Comprehensive Epilepsy Center. "The goal of therapy is the rapid termination of the seizure activity to reduce neurological injuries and deaths."
 From "Treatment of Convulsive Status Epilepticus in Children and Adults" Epilepsy Currents 16.1 January/February 2016. Credit: American Epilepsy Society
From "Treatment of Convulsive Status Epilepticus in Children and Adults" Epilepsy Currents 16.1 January/February 2016. Credit: American Epilepsy Society
Despite recognition of the need to address status epilepticus as a critical care emergency, current treatment approaches vary dramatically. Some therapies focus on reducing rather than ending the seizures and use inefficient therapies such as sedatives and paralytics or insufficient doses of anticonvulsants.
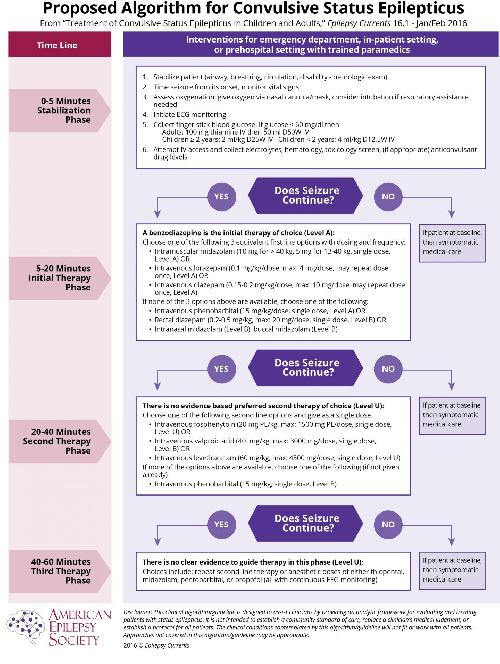
The guideline, which reviewed all available adult and pediatric evidence, provides a treatment algorithm that comprises three phases of treatment. It also offers evidence-based answers to the effectiveness, safety and tolerability questions regarding the treatment of convulsive status epilepticus.
- Stabilization phase (0-5 minutes of seizure activity), includes standard initial first aid for seizures and initial assessments and monitoring.
- Initial therapy phase (5-20 minutes of seizure activity) when it is clear the seizure requires medical intervention, a benzodiazepine (specifically IM midazolam, IV lorazepam, or IV diazepam) is recommended as the initial therapy of choice, given its demonstrated efficacy, safety, and tolerability.
- Second therapy phase (20-40 minutes of seizure activity) when response (or lack of response) to the initial therapy should be apparent. Reasonable options include fosphenytoin, valproic acid and levetiracetam. There is no clear evidence that any one of these options is better than the others. Because of adverse events, IV phenobarbital is a reasonable second-therapy alternative if none of the three recommended therapies are available.
- Third therapy phase (40+minutes of seizure activity). There is no clear evidence to guide therapy in this phase. The guideline found strong evidence that initial second therapy is often less effective than initial therapy, and the third therapy is substantially less effective than initial therapy. Thus, if second therapy fails to stop the seizures, treatment considerations should include repeating second-line therapy or anesthetic doses of either thiopental, midazolam, pentobarbital, or propofol (all with continuous EEG monitoring).
The guideline also found evidence that depending on the causes or severity of the seizure, clinicians may go through the phases faster or even skip the second phase and move rapidly to the third phase, especially in sick or intensive care unit patients.
"In treating status epilepticus there is an overriding urgency to stop seizures before the 30-minute mark when seizure-associated neurologic injury can occur," said guideline coauthor Shlomo Shinnar, M.D., Ph.D., with Albert Einstein College of Medicine and Montefiore Medical Center. "This guideline supports an aggressive approach to treating status epilepticus and seeks to bring some structure to what can often be a chaotic and dire medical situation."
The guideline was endorsed by the Epilepsy Foundation, Child Neurology Society, Association of Child Neurology Nurses, American College of Emergency Physicians and American Association of Neuroscience Nurses.
source: American Epilepsy Society